Care of older
people


Care of older
people


Care of older people
This section includes CPD for geriatricians, geriatric specialist nurses and GPs with an interest in care of older people, including learning on palliative care, neurological conditions, polypharmacy, multimorbidity and other conditions most commonly affecting older people.




Delirium: clinical review


Module description
1.5 CPD hours
This clinical review, updated by Dr Marisa Manning, focuses on the presentation, diagnosis, and management of delirium in secondary care. It also has a case study to explore the management of delirium in a real-world setting.
Educational objectives
After completing this module, healthcare professionals should be better able to:
● Identify the risk factors for delirium
● Describe screening tools for delirium
● Discuss the the management options for delirium
● Understand the probable prognosis for delirium
Definition
Delirium is sometimes referred to as an ‘acute confusional state’. It is a neuropsychiatric syndrome of sudden onset, characterised by altered consciousness, inattention, and disturbances in multiple domains of cognitive function.
The condition usually develops over 24–48 hours and is commonly associated with a reversible medical, surgical, or pharmacological insult to the body. It has a fluctuating course and in many cases, signs of delirium occur more frequently during the evening and night.1
Delirium may occur more frequently
during the evening and night.
References
1. Johansson YA, Bergh I, Ericsson I, Sarenmalm EK. Delirium in older hospitalized patients-signs and actions: a retrospective patient record review. BMC Geriatr 2018; 18(1): 43.





Definition
Delirium is sometimes referred to as an ‘acute confusional state’. It is a neuropsychiatric syndrome of sudden onset, characterised by altered consciousness, inattention, and disturbances in multiple domains of cognitive function.
The condition usually develops over 24–48 hours and is commonly associated with a reversible medical, surgical, or pharmacological insult to the body. It has a fluctuating course and in many cases, signs of delirium occur more frequently during the evening and night.1
Delirium may occur more frequently
during the evening and night.
References
1. Johansson YA, Bergh I, Ericsson I, Sarenmalm EK. Delirium in older hospitalized patients-signs and actions: a retrospective patient record review. BMC Geriatr 2018; 18(1): 43.
Prevalence
Scroll within the image below for information on the prevalence of delirium both in and outside the hospital setting.2,3
Delirium may affect up to 14% of people aged 85 years or older living in the community.
Of people aged 65 years or older presenting to an emergency department, 30% may have delirium.
While in hospital, 10–42% of older adults may have delirium.
70–87% of all people admitted to an intensive care unit may have delirium.
(Image credit: Luis Alvarez/Getty Images)
Delirium may affect up to 14% of people aged 85 years or older living in the community.
Of people aged 65 years or older presenting to an emergency department, 30% may have delirium.
While in hospital, 10–42% of older adults may have delirium.
70–87% of all people admitted to an intensive care unit may have delirium.
(Image credit: Luis Alvarez/Getty Images)
References
2. Vidal EIO, Villas Boas PFJ, Valle AP et al. Delirium in older adults. BMJ 2013: 346: f2031.
3. Raju K, Coombe-Jones M. An overview of delirium for the community and hospital clinician. Prog Neurol Psychiatry 2015; 19(6): 23–7.
Symptoms
At presentation, assess people at risk for recent (within hours or days) changes or fluctuations that may indicate delirium. These may be reported by the person at risk, or a carer or relative. Table 1 (see below) outlines how delirium can affect cognitive, physical, and social functioning.
For the management of delirium red flags in primary care, see the MIMS Learning module by Dr Pipin Singh.
Scroll to view delirium-related changes




Change
Cognitive function
Examples
● Poorer concentration
● Slow responses
● Confusion
Change
Physical function
Examples
● Reduced mobility
● Reduced movement
● Restlessness, agitation
● Changes in appetite
● Sleep disturbance
Change
Social behaviour
Examples
● Difficulty engaging with or following requests
● Withdrawal
● Alterations in communication, mood and/or attitude
Potential causes
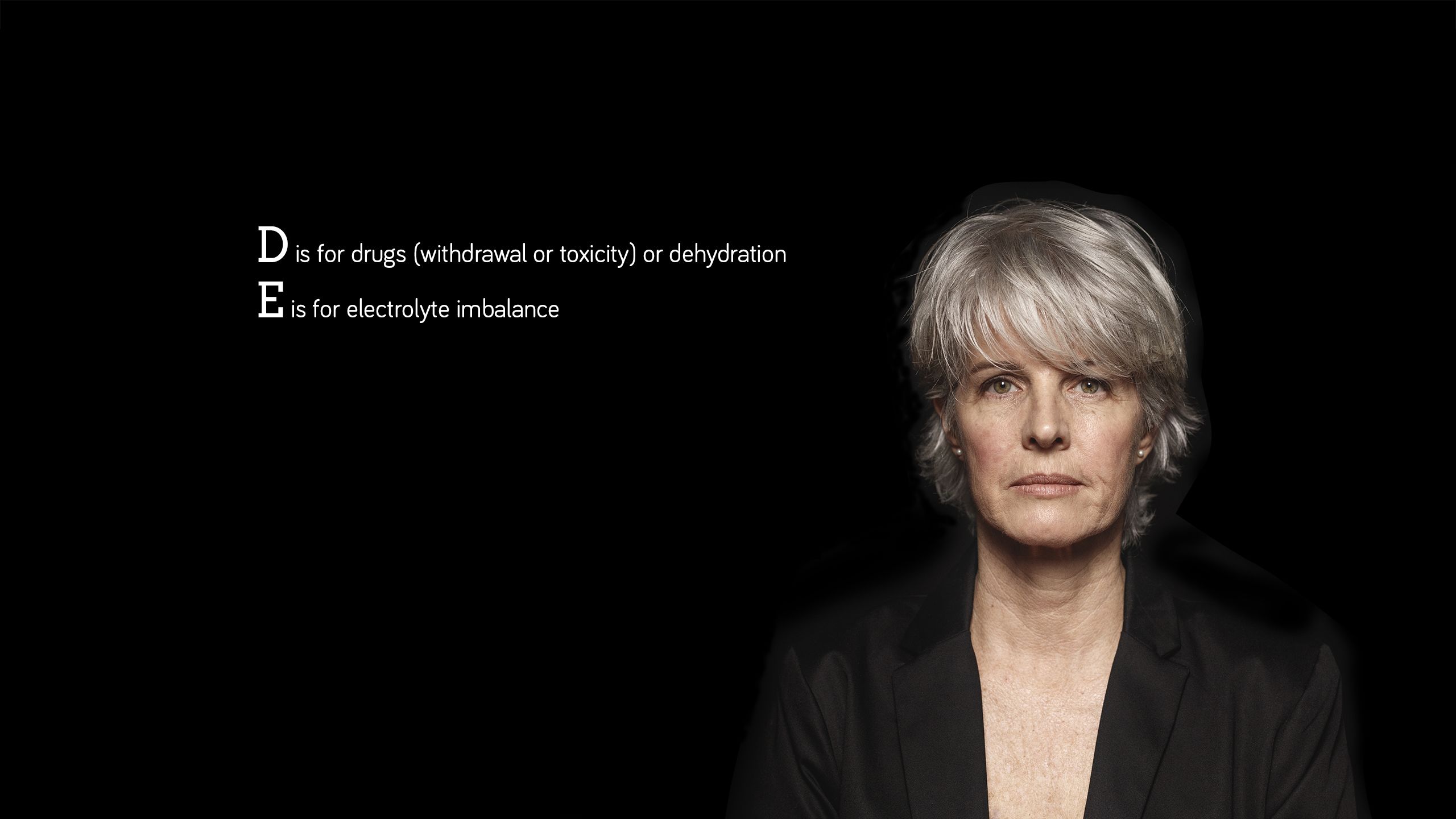
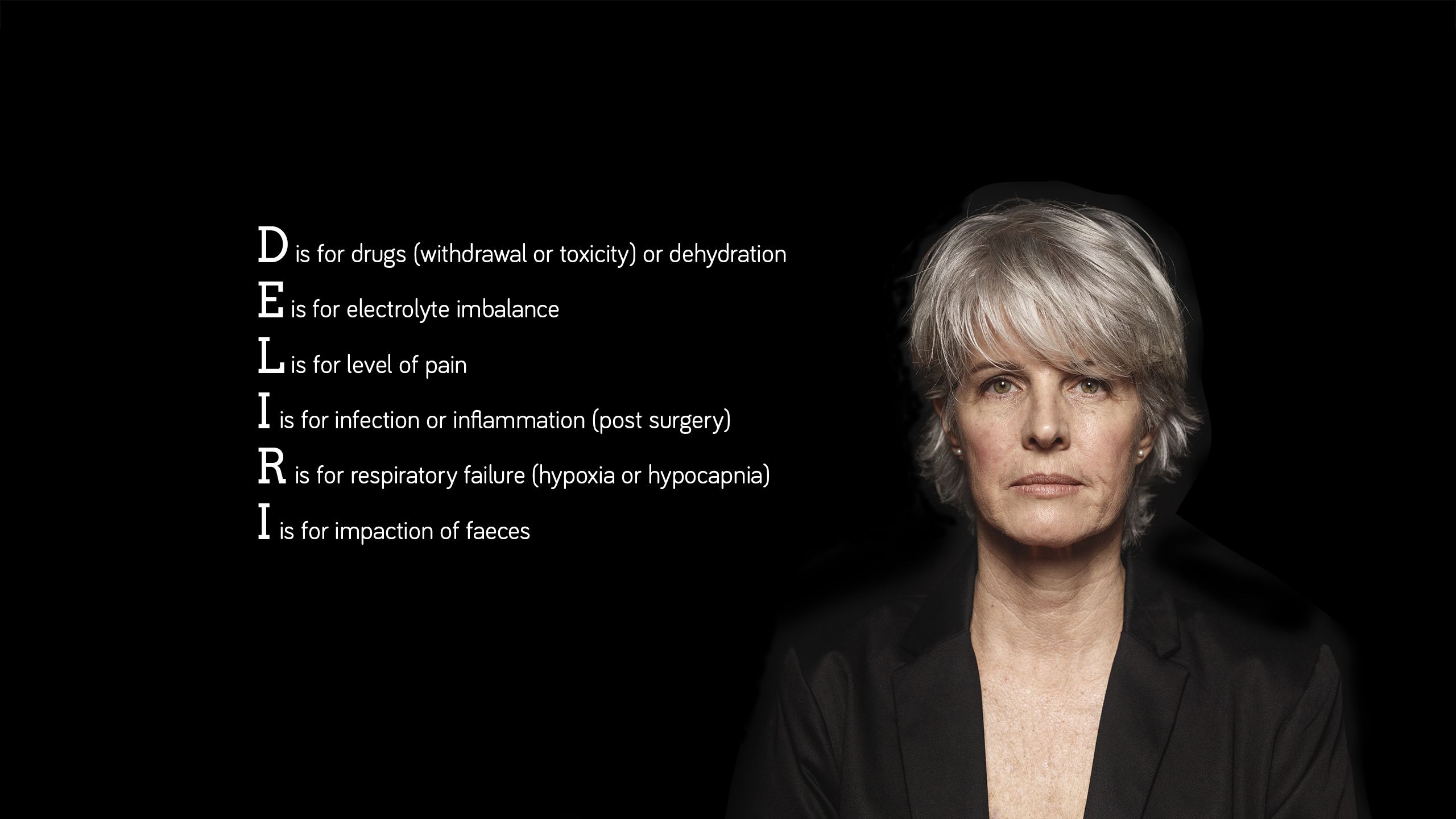
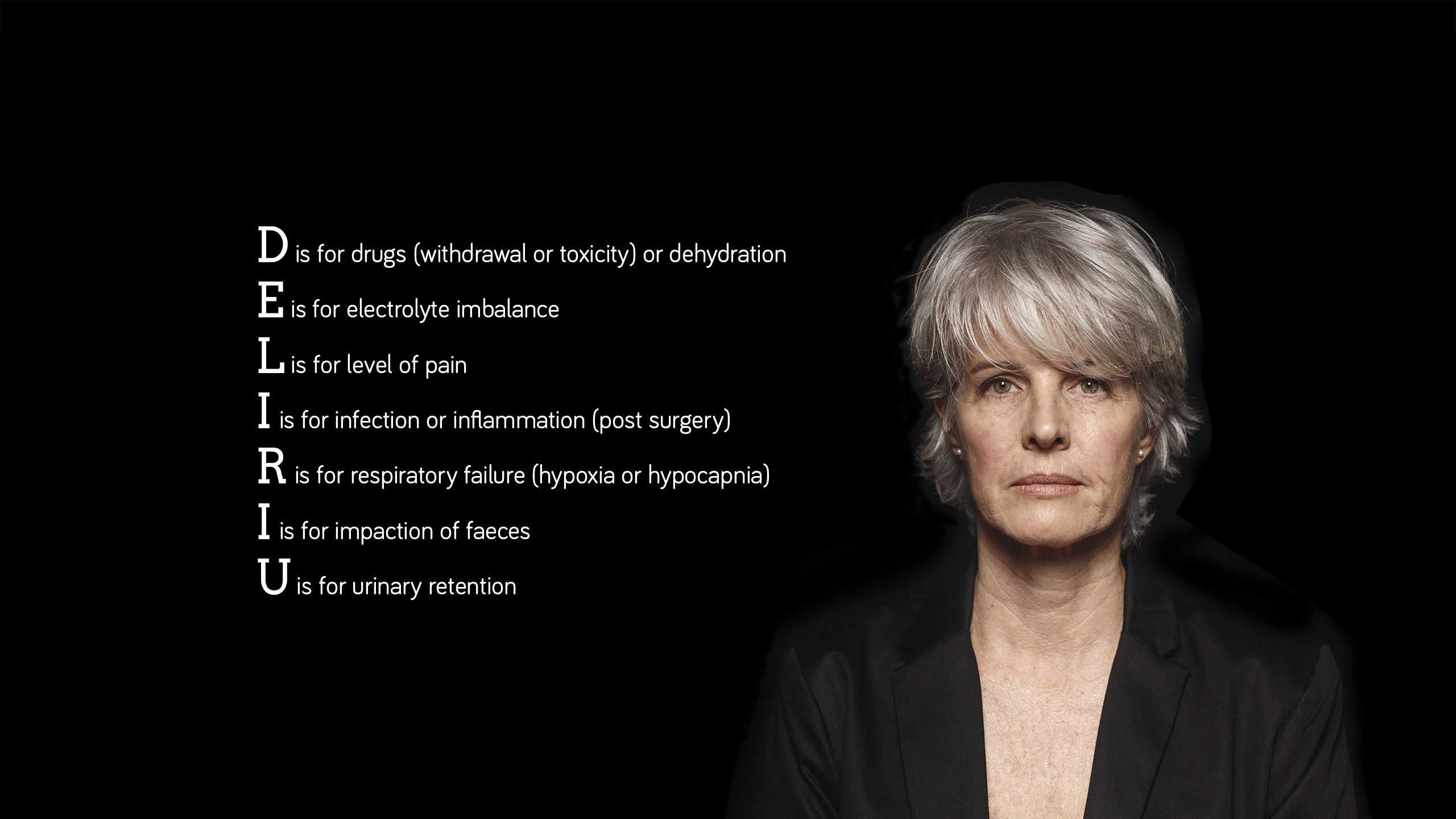
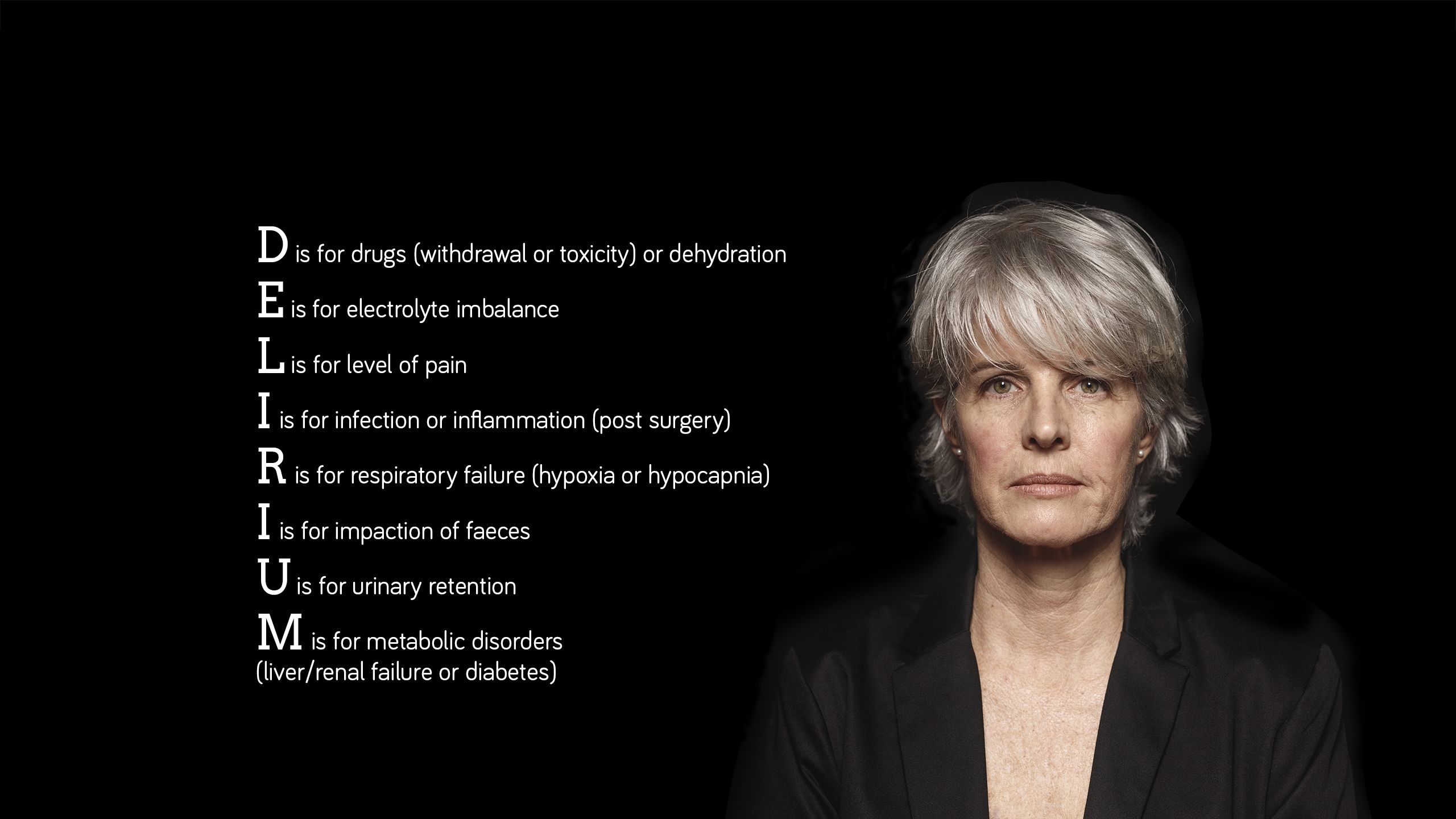
Effective communication with the patient, their family, and colleagues in the multidisciplinary team is key to the effective management of patients with delirium. In distressed and anxious patients, verbal de-escalation should always be first-line.
If a diagnosis of delirium has been established and a cause identified, management should focus on treating the cause. Further management options can be divided into non-pharmacological and pharmacological interventions.
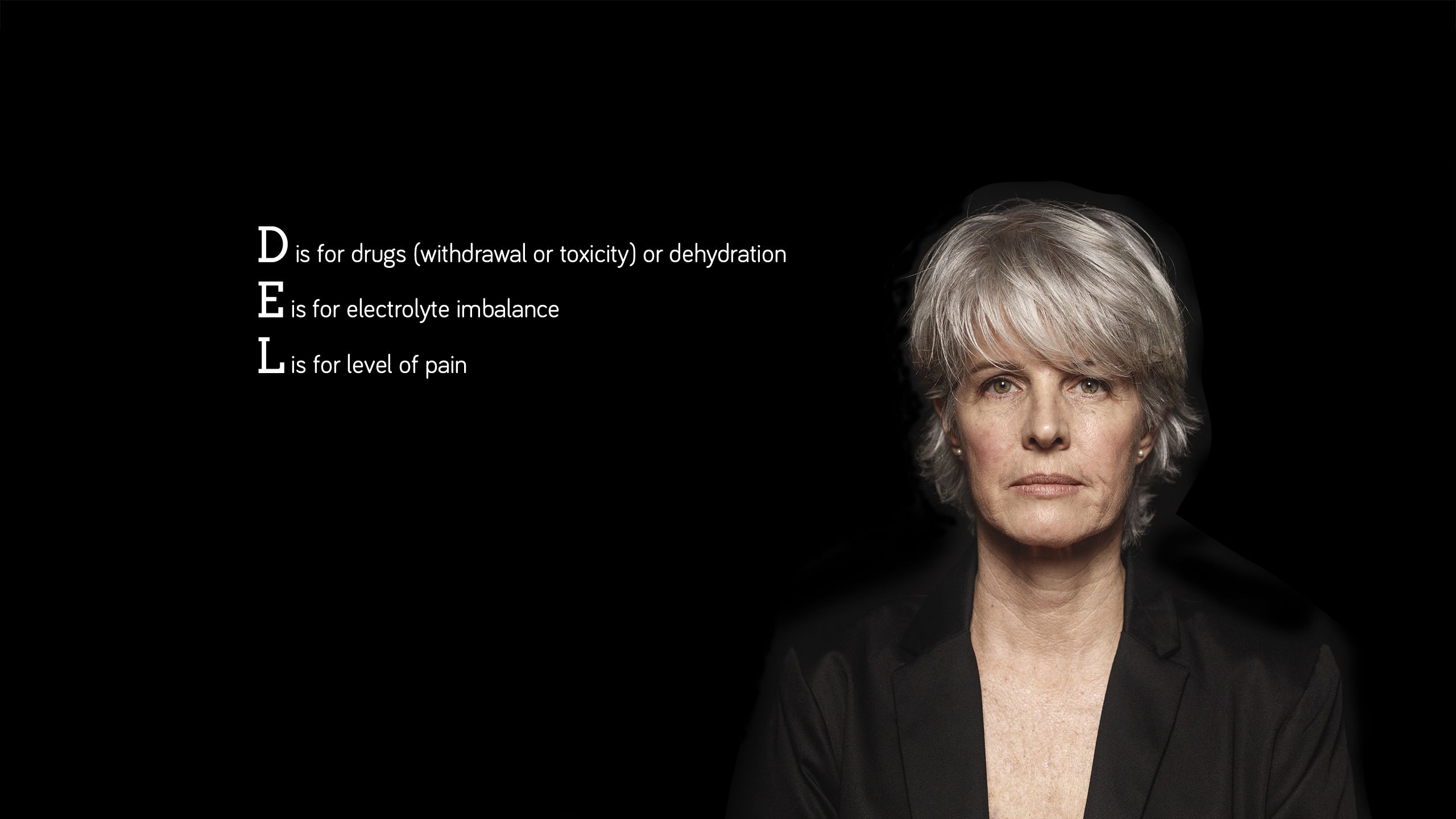
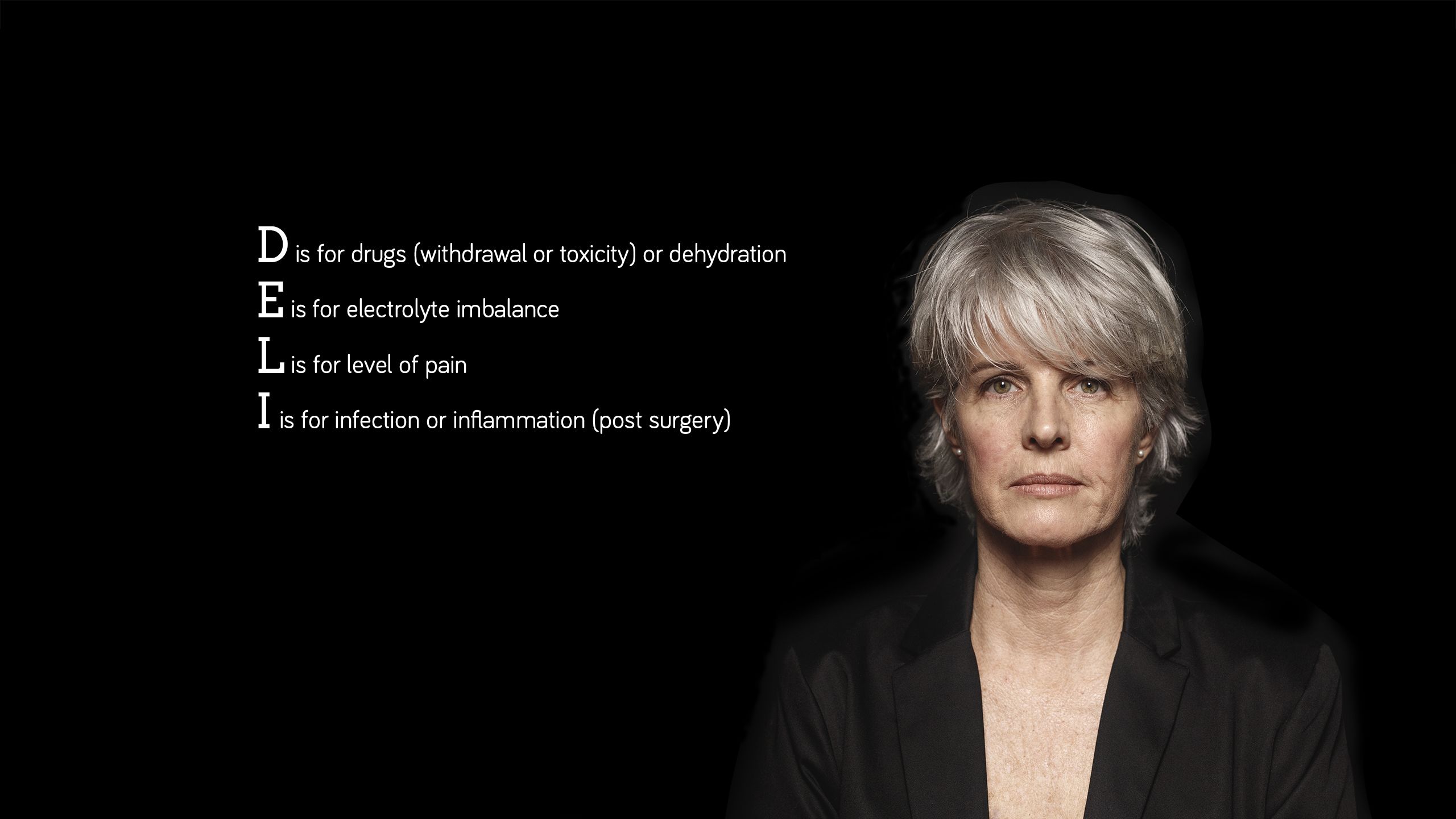
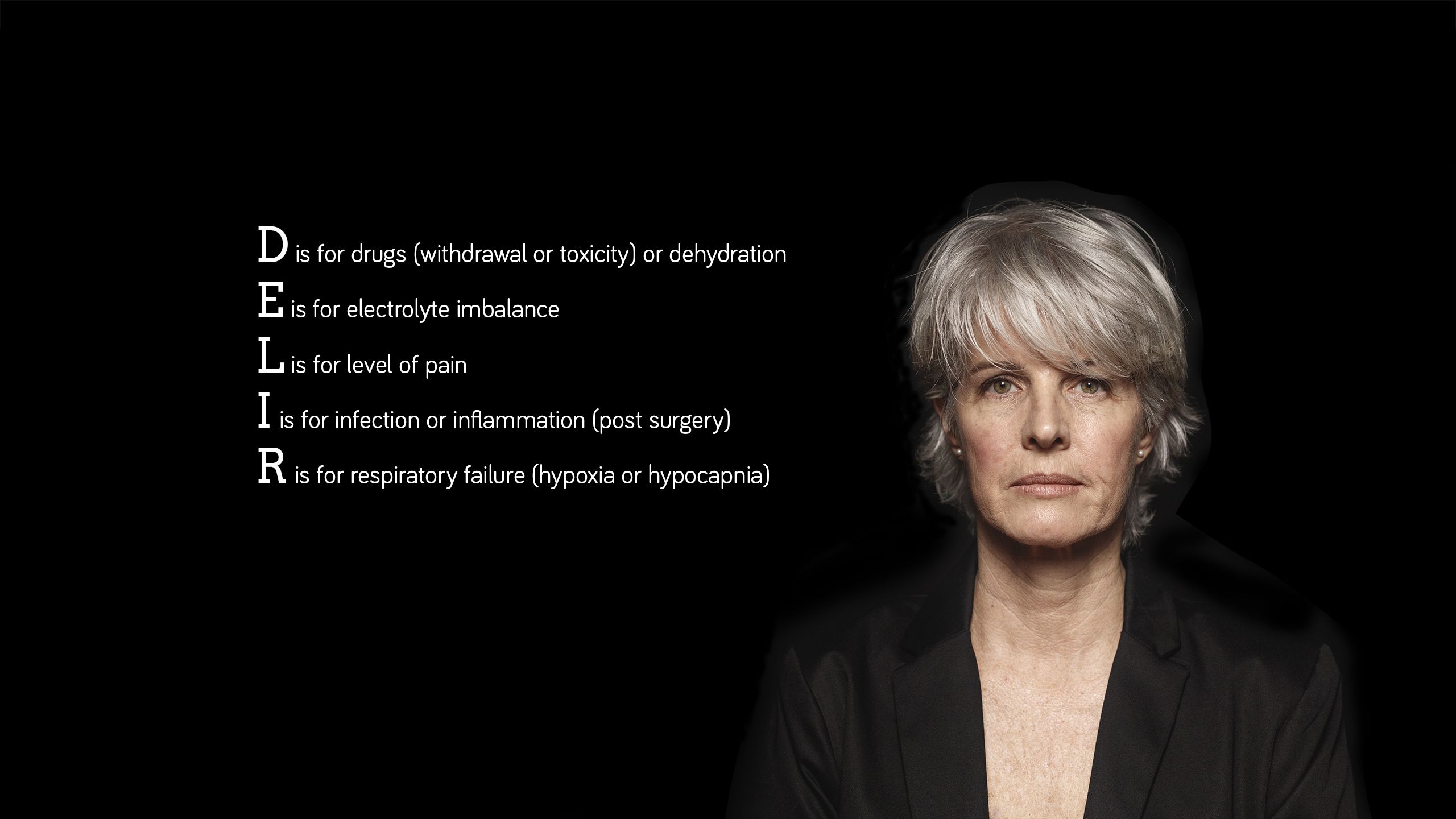
Scroll below to view the ‘DELIRIUM’ mnemonic that can help to identify the cause.











Delirium: clinical review
This clinical review, updated by Dr Marisa Manning, focuses on the presentation, diagnosis, and management of delirium in secondary care. It also has a case study to explore the management of delirium in a real-world setting.
Delirium: clinical review
This clinical review, updated by Dr Marisa Manning, focuses on the presentation, diagnosis, and management of delirium in secondary care. It also has a case study to explore the management of delirium in a real-world setting.


Stroke: clinical review


Module description
1.5 CPD hours
Dr Roser Icart-Palau and Dr Patrick Gompertz outline the epidemiology, aetiology, diagnosis and management of stroke, in a module updated by Dr Pipin Singh. Key learning points for healthcare professionals include the use of the FAST and ABCD2 scores and the cardinal features of clinical presentations of stroke and transient ischaemic attack.
Educational objectives
After reading this activity healthcare professionals should be able to:
● Identify patients at high risk of stroke
● Understand the link between stroke and AF
● Identify high-risk TIA patients
● Recognise the role of early thrombolysis in stroke survival
Prevalence of stroke
There are more than 100,000 strokes in the UK each year.1 Scroll within the image below to find out more.
The number of stroke survivors aged 45+ in the UK is expected to rise by 123% in the next 20 years
Around 1 in 5 women will have a stroke in their life
Around 1 in 6 men will have a stroke in their life
The rate of first time strokes in people aged 45+ is expected to increase by 59% in the next 20 years
The number of stroke survivors aged 45+ in the UK is expected to rise by 123% in the next 20 years
Around 1 in 5 women will have a stroke in their life
Around 1 in 6 men will have a stroke in their life
The rate of first time strokes in people aged 45+ is expected to increase by 59% in the next 20 years
References
1. The Stroke Association. State of the nation: stroke statistics. February 2018.
Making the diagnosis
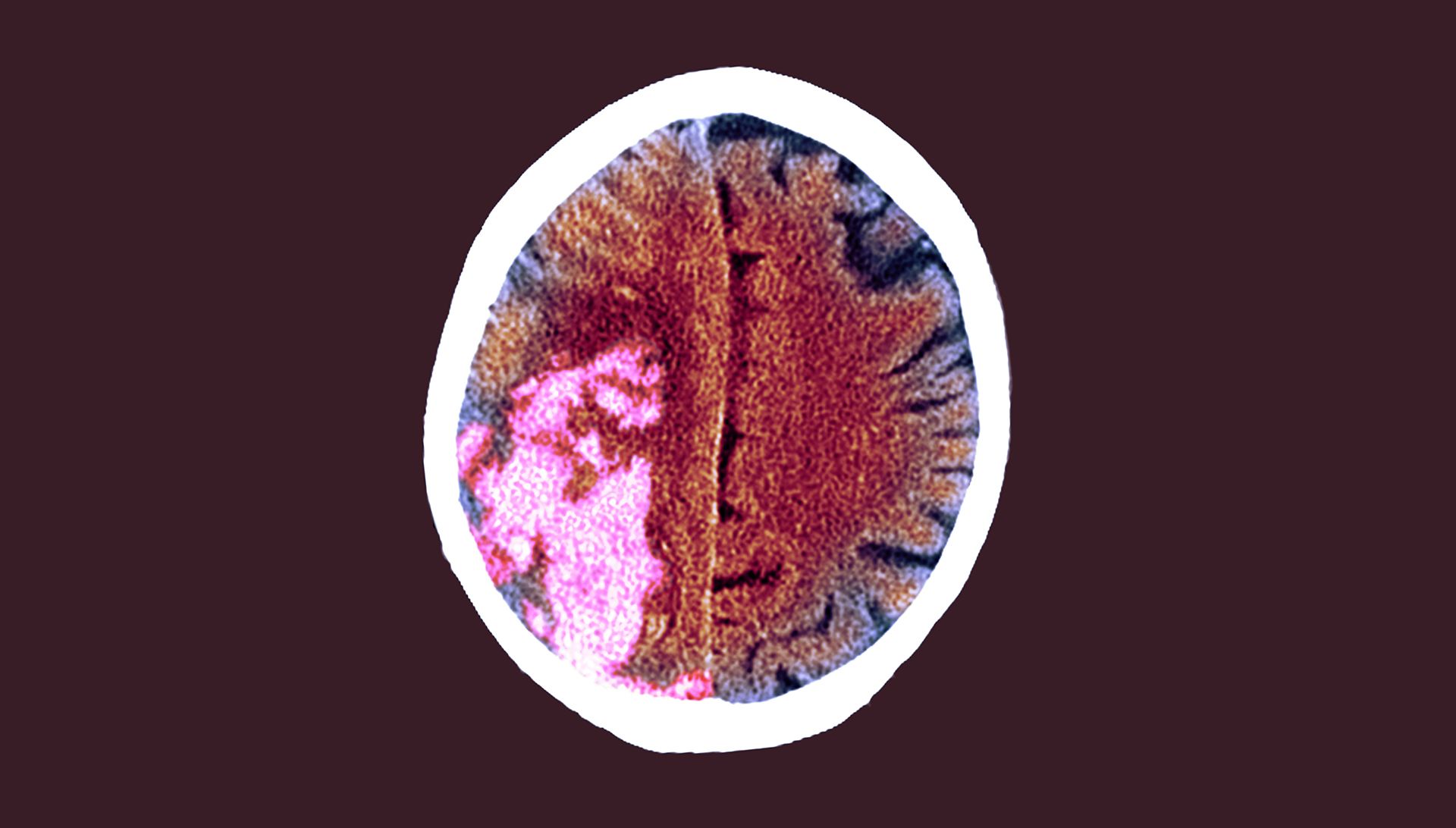
Recognising stroke is very difficult in the acute phase, but essential if patients are to access emergency treatment within the shortest possible time.
FAST (Face, Arms, Speech, Time) is useful as a first assessment test (see box). Approximately 80% of FAST-positive patients will have a confirmed diagnosis of stroke.2,3
Conditions that mimic stroke and can lead to a positive FAST test without being a stroke including seizures, sepsis, metabolic disorders, functional presentations, demyelinating conditions, migraine and space-occupying lesions (SOLs) of the brain.4,5
Scroll within the image below to see FAST signs and symptoms of stroke







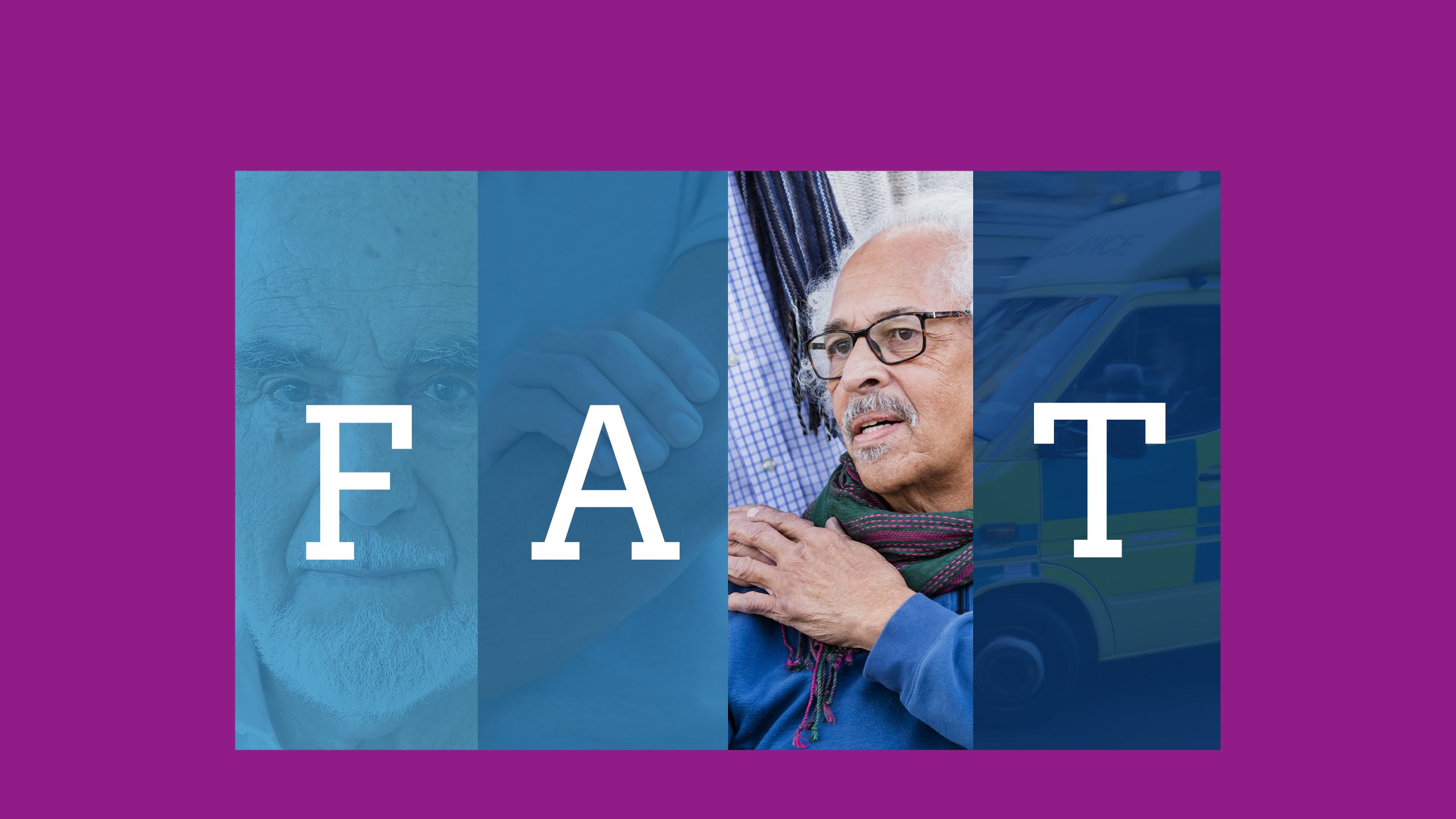


Face
The person’s face may have dropped on one side
(Image credit: Francesco Carta fotografo/Getty Images)
Arms
They may not be able to lift both arms and keep them there because of weakness or numbness in one arm
(Image credit: Science Photo Library/Getty Images)
Speech
Their speech may be slurred or garbled, or they may not be able to talk or understand what you're saying
(Image credit: kali9/Getty Images)
Time
It's time to dial 999 immediately if you notice any of these signs or symptoms
(Image credit: Piccell/Getty Images)
Important!
Approximately 80% of FAST-positive patients will have a confirmed diagnosis of stroke
Important!
Approximately 80% of FAST-positive patients will have a confirmed diagnosis of stroke
References
2. Harbison J, Hossain O, Jenkinson D et al. Diagnostic accuracy of stroke referrals from primary care, emergency room physicians, and ambulance staff using the face arm speech test. Stroke 2003; 34: 71-6.
3. Nor AM, McAllister C, Louw SJ et al. Agreement between ambulance paramedic- and physician-recorded neurological signs with Face Arm Speech Test (FAST) in acute stroke patients. Stroke 2004; 35: 1355-9.
4. Sarikaya H, Yilmaz M, Luft AR et al. Different pattern of clinical deficits in stroke mimics treated with intravenous thrombolysis. Eur Neurol 2012; 68(6): 344-9.
Signs of stroke
Scroll within the images below to reveal the 3 cardinal features of the clinical presentation of stroke or TIA.














Examples of focal neurological symptoms common in stroke are hemiparesis, dysphasia, ataxia, diplopia or visual field loss.
Less focal symptoms and signs include vertigo, amnesia, lightheadedness, loss of consciousness and confusion. These are more likely to be related to another condition, rather than stroke/TIA.5,6
References
5. Nadarajan V, Perry RJ, Johnson J et al. Transient ischaemic attacks: mimics and chameleons. Pract Neurol 2014; 14: 23-31.
6. Nor AM, Davis J, Sen B et al. The Recognition of Stroke in the Emergency Room (ROSIER) scale: development and validation of a stroke recognition instrument. Lancet Neurol 2005; 4(11): 727-34.
Stroke: clinical review
Dr Roser Icart-Palau and Dr Patrick Gompertz outline the epidemiology, aetiology, diagnosis and management of stroke, in an updated learning module for GPs, paramedics and other healthcare professionals, including geriatricians and neurologists.
Stroke: clinical review
Dr Roser Icart-Palau and Dr Patrick Gompertz outline the epidemiology, aetiology, diagnosis and management of stroke, in an updated learning module for GPs, paramedics and other healthcare professionals, including geriatricians and neurologists.


Management of non-melanoma skin cancer in older people

Module description
1 CPD hour
Dr Louise Fearfield discusses the management of non-melanoma skin cancer in older people and recommends an individualised approach to treatment.
Educational objectives
After completing this activity, healthcare professionals should be better able to:
● Recall the prevalence of non-melanoma skin cancer (NMSC) in older people
● Understand the projected increase of NMSC among elderly people
● Reflect on current treatment of BCC and SCC
● Understand why elderly patients may need an individualised approach
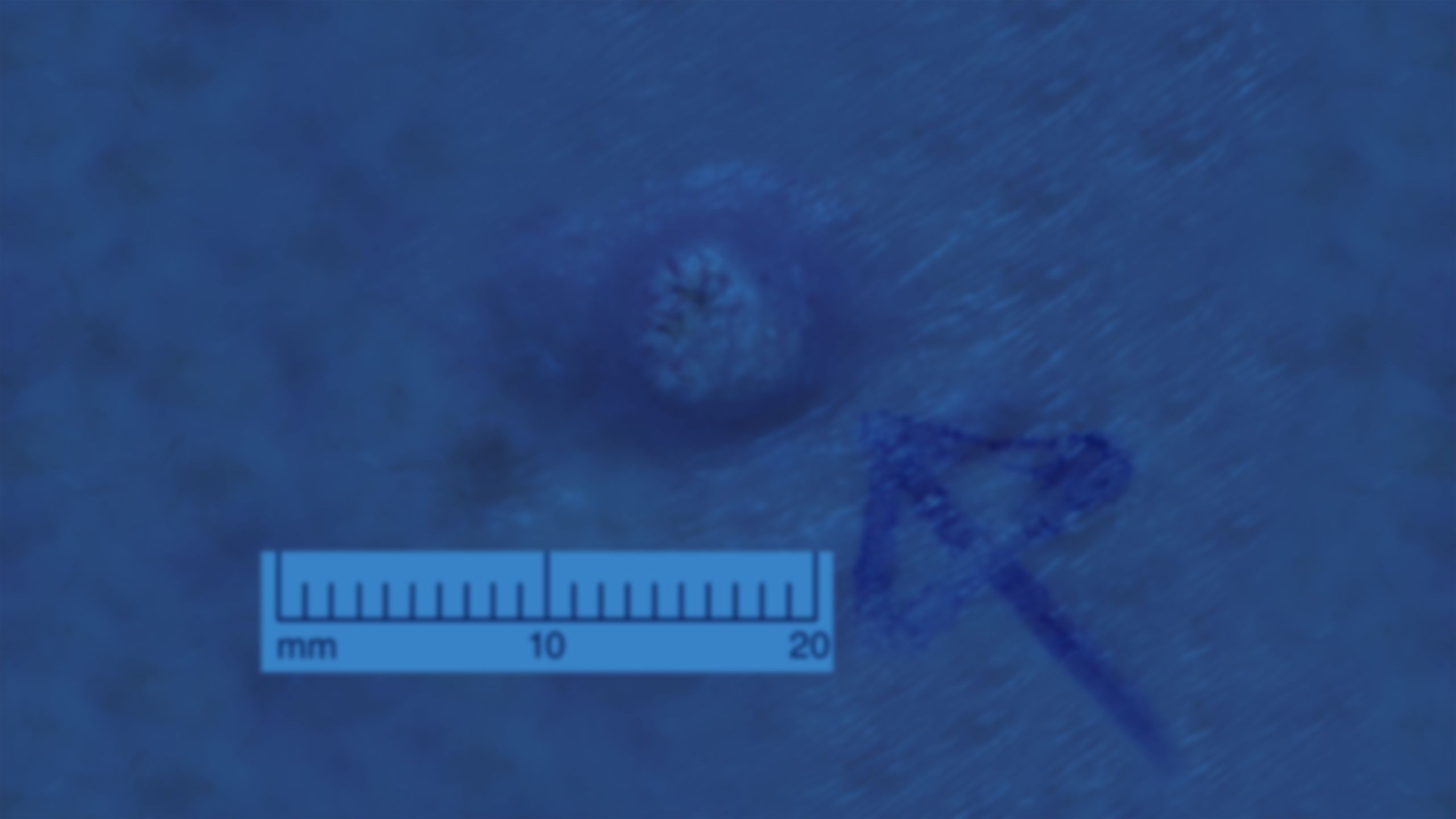
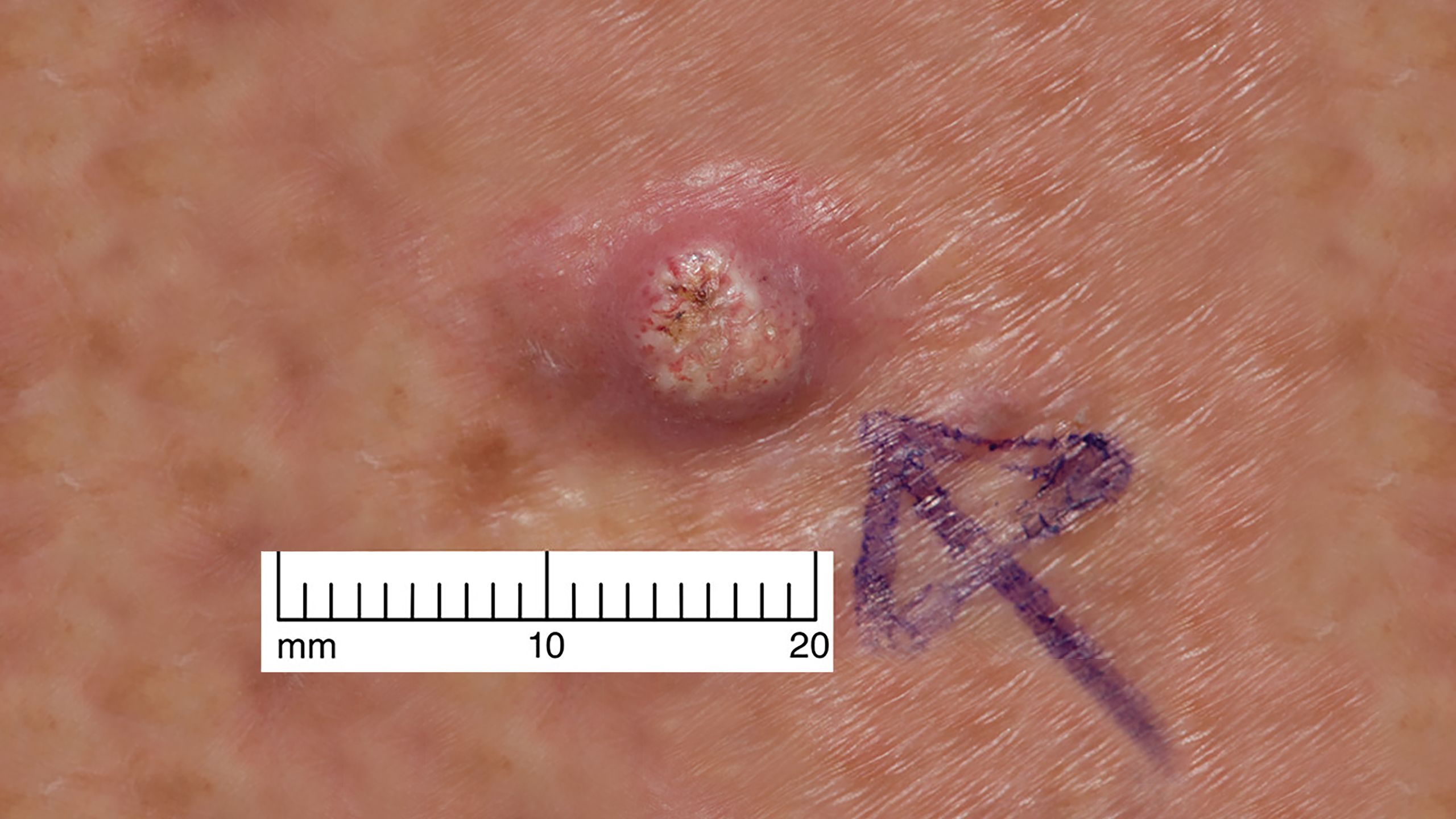
Skin cancer facts and figures
Scroll within the image below to find out more about skin cancer, the most common malignancy in the UK.














References
1. National Cancer Institute. Age and cancer risk. April 29, 2015.
2. White M, Holman D, Boehm J et al. Age and cancer risk. Am J Prev Med 2014; 46: S7-15.
Alternatives to surgery
Low-risk BCCs can be managed well using destructive modalities such as electrodessication and curettage, and cryosurgery. Electrodessication and curettage is a fast and inexpensive treatment for BCCs, but it does not allow for histological confirmation of the tumour clearance, and its use is virtually limited to low-risk BCCs due to high recurrence rates.
Topical therapies including 5% imiquimod and fluorouracil are also used to treat low-risk tumours but generally not higher-risk lesions. Kaçar et al reported four cases of high-risk BCCs in elderly patients, successfully treated with 12 weeks daily or alternate days of 5% imiquimod, who were not suitable for other treatment modalities. BCCs treated including a 2cm ulcerated nodular BCC on the nose and lip.12


Radiation therapy can be used as primary or adjuvant therapy in NMSCs, and provides an alternative treatment option if surgery is contraindicated or undesirable. Marriappan et al treated 25 elderly patients with BCC and a mean age of 89 (range 83-103) with weekly radiotherapy (42Gy in seven fractions over seven weeks). 84% of BCCs were >2cm at presentation.13
All patients completed treatment and at 6 weeks post-treatment, 92% had a complete or good partial response. At 15-month follow-up, 11 patients were still alive. This regime would not be recommended for younger patients due to the potential long-term effects of large fractionation sizes on normal tissue.


Radiotherapy can be used as a primary or adjuvant therapy
(Image credit: Mark Kostich/Getty Images)
References
12. Kaçar SD, Özuğus P, Erkan F, Karaca Ş. Treatment of various types of basal cell carcinoma with topical 5% imiquimod in the elderly who refused surgical intervention: a case series. J Dermatol Treatment 2015; 26 (2): 165-7.
13. Marriappan L, Ramasamy S, Robert F. Weekly radiotherapy for basal cell carcinoma in the frail and elderly. Br J Dermatol 2014; 171 (5); 1237-9.
Key learning points

The incidence of skin cancer is highest in people over the age of 85

Many patients with shorter life expectancy are not troubled by BCCs and may die of causes unrelated to skin cancer

Older patients are at risk of surgery-related complications

Treatment for older patients should aim to improve overall well-being, taking functional age and comorbidities into account

Management of non-melanoma skin cancer in older people
Dr Louise Fearfield discusses the management of non-melanoma skin cancer in older people and recommends an individualised approach to treatment.
Management of non-melanoma skin cancer in older people
Dr Louise Fearfield discusses the management of non-melanoma skin cancer in older people and recommends an individualised approach to treatment.

End of life care: a guide for GPs and nurses
0.5 CPD hours
This learning module by Dr Anish Kotecha offers advice for GPs, GP trainees, nurses and allied healthcare professionals on managing patients at the end of life.
Educational objectives
After reading this activity, healthcare professionals should be better able to:
● Identify patients who are approaching the end of their life
● Communicate effectively with patients and their families about advance care plans
● Conduct a holistic assessment encompassing the patient’s physical, psychological, social, and spiritual needs
● Manage common symptoms such as breathlessness, nausea and agitation

Assessment of older people
1 CPD hour
In a learning module for GPs and geriatricians, Dr Pipin Singh provides insight into the pitfalls of assessing older patients and presents case studies of good multidisciplinary care.
Educational objectives
After undertaking this activity, healthcare professionals should be better able to:
● Assess older patients taking into account factors such as physical symptoms and signs
● Conduct assessments appropriately in different settings including the patient’s home
● Be aware of common drug side-effects
● Be aware of the Mental Capacity Act and the potential role of advocates

Guidance update: NOGG guidelines on osteoporosis
1 CPD hour
This updated learning module describes current guidance from the National Osteoporosis Guidelines Group (NOGG) on diagnosis, management and referral of osteoporosis.
Educational objectives
After taking this module, GPs and nurses will be better able to:
● Recall what’s relevant to them in the NOGG guidance on osteoporosis
● Describe the clinical indicators that point to a diagnosis of osteoporosis
● Know which patients should be treated without further investigation and which need referral for DEXA scanning
● Carry out investigations to exclude secondary causes of osteoporosis
● Give appropriate lifestyle advice to patients at risk of osteoporosis

Recurrent falls in older people
0.75 CPD hours
Consultant in geriatrics and general medicine Dr Anna Steel provides tips on identifying causes of recurrent falls in older people, and preventing further falls, in a webinar recorded for MIMS Learning Live Digital.
Educational objectives
After viewing this webinar, healthcare professionals should be better able to:
● Understand why people fall
● Assess falls in the GP setting
● Recommend holistic modifications to reduce falls risk
● Deprescribe and recommend exercise
Sign up for MIMS Learning Live in London here.
End of life care: a guide for GPs and nurses
0.5 CPD hours
This learning module by Dr Anish Kotecha offers advice for GPs, GP trainees, nurses and allied healthcare professionals on managing patients at the end of life.
Educational objectives
After reading this activity, healthcare professionals should be better able to:
● Identify patients who are approaching the end of their life
● Communicate effectively with patients and their families about advance care plans
● Conduct a holistic assessment encompassing the patient’s physical, psychological, social, and spiritual needs
● Manage common symptoms such as breathlessness, nausea and agitation
Assessment of older people
1 CPD hour
In a learning module for GPs and geriatricians, Dr Pipin Singh provides insight into the pitfalls of assessing older patients and presents case studies of good multidisciplinary care.
Educational objectives
After undertaking this activity, healthcare professionals should be better able to:
● Assess older patients taking into account factors such as physical symptoms and signs
● Conduct assessments appropriately in different settings including the patient’s home
● Be aware of common drug side-effects
● Be aware of the Mental Capacity Act and the potential role of advocates
Guidance update: NOGG guidelines on osteoporosis
1 CPD hour
This updated learning module describes current guidance from the National Osteoporosis Guidelines Group (NOGG) on diagnosis, management and referral of osteoporosis.
Educational objectives
After taking this module, GPs and nurses will be better able to:
● Recall what’s relevant to them in the NOGG guidance on osteoporosis
● Describe the clinical indicators that point to a diagnosis of osteoporosis
● Know which patients should be treated without further investigation and which need referral for DEXA scanning
● Carry out investigations to exclude secondary causes of osteoporosis
● Give appropriate lifestyle advice to patients at risk of osteoporosis
Recurrent falls in older people
0.75 CPD hours
Consultant in geriatrics and general medicine Dr Anna Steel provides tips on identifying causes of recurrent falls in older people, and preventing further falls, in a webinar recorded for MIMS Learning Live Digital.
Educational objectives
After viewing this webinar, healthcare professionals should be better able to:
● Understand why people fall
● Assess falls in the GP setting
● Recommend holistic modifications to reduce falls risk
● Deprescribe and recommend exercise
Sign up for MIMS Learning Live in London here.