Mental health


Mental health


Mental health and psychiatry
This section has CPD modules for healthcare professionals with an interest in mental health and psychiatry (including psychiatrists and psychiatric nurse specialists). It has modules on anxiety, depression, eating disorders, and attention deficit hyperactivity disorder (ADHD), and also has content on child and adolescent mental health.
Dr Muffazal Rawala
Consultant psychiatrist at East London NHS Foundation Trust




Depression: clinical review



Module description
1.5 CPD hours
In this clinical review, Dr Mario F Juruena looks at the different subtypes of depression — ranging from melancholic depression to psychotic depression. He also discusses prevalence, management options, and prognosis.
Educational objectives
After taking this activity healthcare professionals should be better able to:
● Understand the aetiology and epidemiology of depression
● Describe the subtypes of depression and how they present
● Review management options for people with depression
● Discuss the rate of recurrence of depressive episodes
Introduction
A fundamental challenge with mood disorders is that the classification of different types of mood disorders, including clinical subtypes, is based on subjective descriptions of symptoms. This is because, at present, the evidence for biological characteristics that could be used to differentiate one type from another is insufficient.
Additional challenges are that a variety of depressive and bipolar disorders can exhibit similar clinical symptoms and that the same condition can manifest itself differently in different people — or even differently in the same person at different times.
Thus, there is a need for greater knowledge in diagnosing mood disorders. The main objective of this module is to focus on the categorisation, identification, and management of depressive disorders.

Prevalence
Scroll within the image below to view prevalence data about depression.
Depression is two to three times more common in women than it is in men (affecting 10–25% of women and 5–12% of men).1 Gender differences in the incidence of depression begin to emerge between 13 and 15 years of age, becoming more evident between 15 and 18 years of age.
The incidence of depression is at its highest between the ages of 25 and 30, but depression can occur at any age and stage of life.1,2 Also, the incidence seems to be increasing among children and adolescents.
Depression is the second most common cause of sick leave because of disability in developed countries and the first in developing countries.2
Depressive disorders are significantly associated with exposure to traumatic events.4
The average duration of an episode of depression is between 16 and 20 weeks, and 12% of patients have a chronic course without remission of symptoms.3
Primary care data show a consistently rising number of people under 40 years being diagnosed with type 2 diabetes.2
Although people with YOT2D only represent a small proportion (4%) of the overall diabetes population, the incidence of YOT2D is increasing at a faster rate than that of type 2 diabetes of typical onset: 23% versus 18%, respectively, between the years 2016/2017 and 2019/2020.3,4
According to the Global Burden of Diseases study, the incidence of YOT2D in the UK is rising faster than anywhere else in the world.5
The risk of YOT2D increases with age, with most cases occurring between the ages of 26 and 39 (only 1.3% of cases occur in people aged 18 years or younger).3
A 2023 diabetes audit found that there are now more people in England under the age of 40 with type 2 diabetes than those with type 1 diabetes.
References
1. Kessler RC, Berglund P, Demler O et al. National Comorbidity Survey Replication. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003; 289(23): 3095–105.
2. Moussavi S, Chatterji S, Verdes E et al. Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet 2007; 370(9590): 851–8.
3. Souery D, Oswald P, Massat I et al. Clinical factors associated with treatment resistance in major depressive disorder: results from a European multicenter study. J Clin Psychiatry 2007; 68(7): 1062–70.
4. Andrade LH, Wang Y-P, Andreoni S et al. Mental disorders in megacities: findings from the São Paulo megacity mental health survey, Brazil. PLoS One 2012; 7(2): e31879.
Genetics
Scroll within the image below to view how genetics affects depression.












Both bipolar disorder and major depressive disorder are highly heritable conditions, with heritability estimates ranging as high as 85–93% and 40–50%, respectively.6
In fact, depression is associated with various biological abnormalities including:5
Vascular changes
Changes in autonomic function
Hypercoagulability
Hyperactivity of the hypothalamic-pituitary-adrenal (HPA) axis
Both bipolar disorder and major depressive disorder are highly heritable conditions, with heritability estimates ranging as high as 85–93% and 40–50%, respectively.6
In fact, depression is associated with various biological abnormalities including:5
Vascular changes
Changes in autonomic function
Hypercoagulability
Hyperactivity of the hypothalamic-pituitary-adrenal (HPA) axis
Several studies have found that children of people with depression are at greater risk of developing earlier, more severe, and recurrent depression than children of people without depression. Additionally, an identical twin has a 50% to 80% chance of having the same depressive disorder as their sibling.1,5,7
However, the specific genetic characteristics of major depressive disorder (and bipolar disorder) remain relatively unknown, with recent studies pointing to complex, multifactorial, and highly polygenic architectures. Additionally, as previously mentioned, environmental factors are also important.


An identical twin has a 50% to 80%
chance of having the same depressive
disorder as their sibling
(Image credit: Emily Stein/Getty Images)
References
1. Kessler RC, Berglund P, Demler O et al. National Comorbidity Survey Replication. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003; 289(23): 3095–105.
5. Juruena MF. Early-life stress and HPA axis trigger recurrent adulthood depression. Epilepsy Behav 2014; 38C: 148–59.
6. Menezes IC, von Werne Baes C, Lacchini R, Juruena MF. Genetic biomarkers for differential diagnosis of major depressive disorder and bipolar disorder: a systematic and critical review. Behav Brain Res 2019; 357–8:29–38.
7. Menezes IC, von Werne Baes C, Fígaro-Drumond FV et al. Differential diagnosis of major depressive disorder and bipolar disorder: genetic and hormonal assessment and the influence of early-life stress. Brain Sciences 2022; 12(11): 1476.

Depression: clinical review
In this clinical review, Dr Mario F Juruena looks at the different subtypes of depression — ranging from melancholic depression to psychotic depression. He also discusses prevalence, management options, and prognosis.

Depression: clinical review
In this clinical review, Dr Mario F Juruena looks at the different subtypes of depression — ranging from melancholic depression to psychotic depression. He also discusses prevalence, management options, and prognosis.


Tourette syndrome and other tic disorders in children and adolescents


Module description
1.0 CPD hour
In this educational module for psychiatrists and other healthcare professionals with an interest in mental health, Olivia Horner, Dr Tammy Hedderly, and Dr Osman Malik look at Tourette syndrome (TS) and other tic disorders in children and adolescents. They review aetiology, diagnosis, and management options.
Educational objectives
After taking this activity healthcare professionals should be better able to:
● Discuss the differences between TS and other tic disorders
● Describe the comorbid conditions that are commonly associated with TS
● Understand what questions to ask to determine if behaviours relate to a tic disorder
● Review the different treatment options for TS
Introduction
Tics
Tics refer to movements or vocalisations that are sudden, rapid, repetitive and usually ‘irresistible’ (which is different from ‘involuntary’).1 With tics, there is often the presence of a strong ‘premonitory urge’ (a feeling of inner tension or awareness that the tic is about to emerge); however, a person may be able to delay performing the tic for a brief period of time or may be able to replace it with a smaller movement/vocalisation.2
Tourette syndrome
The name ‘Tourette’ comes from the French doctor Georges Gilles de la Tourette, who published a paper on chronic tics in the 19th century. However, it was Dr Jean-Martin Charcot who coined the term ‘Tourette’s syndrome’ in honour of de la Tourette (however, Charcot gave his name to several other conditions).3


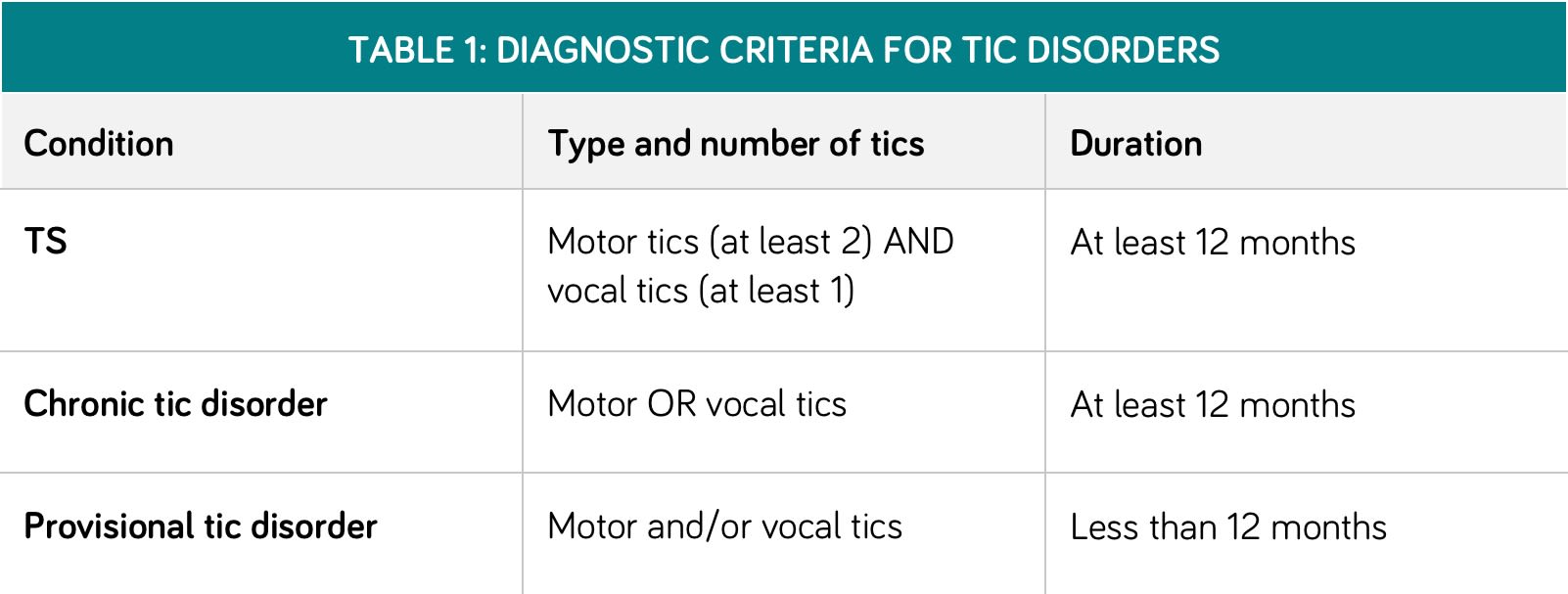
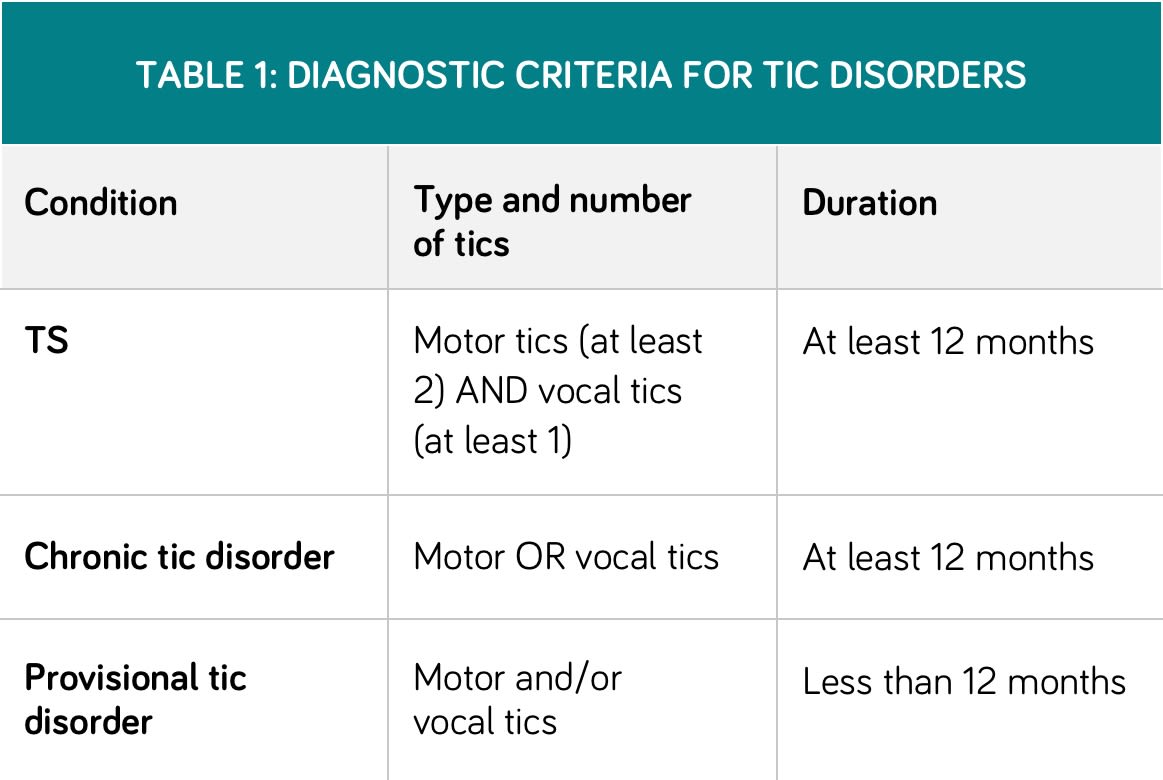
Table 1 (below) outlines the diagnostic criteria for Tourette syndrome (TS), chronic tic disorder, and provisional tic disorder. Of note, these definitions require an onset of tics before age 18 years and need the exclusion of other causes (such as Huntington’s disease) and/or drug side-effects.4

References
1. NHS. Tourette's syndrome. Accessed October 2022.
2. Malik O, Hedderly T. Childhood tic disorders: diagnosis and management. Paediatr Child Health 2018; 28: 445–53.
3. Wikipedia. Tourette syndrome. Accessed October 2022.
4. Centers for Disease Control and Prevention. Diagnosing tic disorders. Accessed October 2022.
Facts and figures
Tic disorders are common in children, with about 1% of children experiencing TS or chronic tic disorder (TS alone affects 0.6% of children).5 Age of onset is usually between 4 and 7 years, and the average age of onset is 6 years.1
Tics can wax and wane over time and can move around to different parts of the body. Therefore, new tics may emerge and some existing ones may ‘disappear’. This is not a sign of progression but rather the expected course of tic conditions. However, tics will completely disappear by late teens/early adulthood in about 55–60% of young people.6
Non-TS healthcare professionals need to be aware of tic disorders as children can present in many settings, including general practice, the emergency department, or in specialist clinics. For example, those with coughs, sniffing or eye-scrunching tics could present in ophthalmology, ENT, respiratory, or allergy clinics.
Scroll within the image below to view more facts and figures about tics
Table 1 (below) outlines the diagnostic criteria for Tourette syndrome (TS), chronic tic disorder, and provisional tic disorder. Of note, these definitions require an onset of tics before age 18 years and need the exclusion of other causes (such as Huntington’s disease) and/or drug side-effects.4

References
1. NHS. Tourette's syndrome. Accessed October 2022.
2. Malik O, Hedderly T. Childhood tic disorders: diagnosis and management. Paediatr Child Health 2018; 28: 445–53.
3. Wikipedia. Tourette syndrome. Accessed October 2022.
4. Centers for Disease Control and Prevention. Diagnosing tic disorders. Accessed October 2022.
Facts and figures
Tic disorders are common in children, with about 1% of children experiencing TS or chronic tic disorder (TS alone affects 0.6% of children).5 Age of onset is usually between 4 and 7 years, and the average age of onset is 6 years.1
Tics can wax and wane over time and can move around to different parts of the body. Therefore, new tics may emerge and some existing ones may ‘disappear’. This is not a sign of progression but rather the expected course of tic conditions. However, tics will completely disappear by late teens/early adulthood in about 55–60% of young people.6
Non-TS healthcare professionals need to be aware of tic disorders as children can present in many settings, including general practice, the emergency department, or in specialist clinics. For example, those with coughs, sniffing or eye-scrunching tics could present in ophthalmology, ENT, respiratory, or allergy clinics.
Scroll within the image below to view more facts and figures about tics
Repetitive blinking, throat clearing or sniffing tend to be the first tics.
Tics are usually at their peak severity between ages 10 and 12; after 13, they tend to reduce in a fluctuating manner.7
If tics do persist into adulthood, they are minor or minimal for 20–25% of people. However, another 20% may continue to have tics with some severity.6
Only about 15–20% of people with TS will experience coprolalia (inappropriate or swear words).8
Repetitive blinking, throat clearing or sniffing tend to be the first tics.
Tics are usually at their peak severity between ages 10 and 12; after 13, they tend to reduce in a fluctuating manner.7
If tics do persist into adulthood, they are minor or minimal for 20–25% of people. However, another 20% may continue to have tics with some severity.6
Only about 15–20% of people with TS will experience coprolalia (inappropriate or swear words).8
References
1. NHS. Tourette's syndrome. Accessed October 2022.
5. Tourette’s Association of America. The spectrum of Tourette syndrome and tic disorders: a consensus by scientific advisors of the Tourette Association of America. March 2017.
6. Exploring your mind. Tics in childhood: characteristics and treatment. October 2019.
7. Hassan N, Cavanna AE. The prognosis of Tourette syndrome: implications for clinical practice. Funct Neurol 2012; 27(1): 23–7.
8. Horner O, Hedderly T, Malik O. The changing landscape of childhood tic disorders following COVID-19. Paediatr Child Health (Oxford) 2022; 32(10): 363–7.
Types of tics
Tics can be grouped, somewhat arbitrarily, into ‘simple’ and ‘complex’. Simple and complex tics (categorised into motor and vocal tics) are compared below. A more extensive list of tics can be found in the Yale Global Tic Severity Scale, which is used for assessment of children with tic disorders.
Scroll within the image below to view more about simple tics versus complex tics.




Motor
Simple
Motor movements involving only one muscle group. For example:
● Shoulder shrugging
● Eye blinking
● Face grimacing
Complex
Multiple muscle groups and may follow some sort of pattern or purpose. For example:
● Reaching out for objects
● Doing multiple movements in quick succession
Vocal
Simple
‘Random’ sounds, including:
● Grunting
● Syllables
Complex
● Coprolalia (swearing, inappropriate language)
● Echos
● Repeating full words and sentences
Motor
Simple
Motor movements involving only one muscle group. For example:
● Shoulder shrugging
● Eye blinking
● Face grimacing
Complex
Multiple muscle groups and may follow some sort of pattern or purpose. For example:
● Reaching out for objects
● Doing multiple movements in quick succession
Vocal
Simple
‘Random’ sounds, including:
● Grunting
● Syllables
Complex
● Coprolalia (swearing, inappropriate language)
● Echos
● Repeating full words and sentences
Important!
Remember that despite its over-representation in the media, coprolalia only affects 15–20% of people with TS
Medication
Medications for tics can be considered if the child is experiencing severe or debilitating tics or muscular pains from repetitive actions.
First-line medication for tics in children include alpha-agonists such as clonidine and guanfacine.9 Alternatively, antidopaminergic medications such as aripiprazole can be helpful. There are other novel and experimental approaches to managing tics, such as Botox and deep brain stimulation, but these are seldom used in children and adolescents.
The choice of medications sometimes depends on the comorbidity. For instance, aripiprazole may be best for a child with emotional regulation problems and rage with the tics; on the other hand, clonidine may be better for a child with severe sleep problems with the tics.
Tics that are resistant to treatment often require a reformulation of the issue and understanding factors that may be maintaining tics, such as:








Stress
Anxiety
Substances/ drugs
Excessive use of energy drinks
Stress
Anxiety
Substances/ drugs
Excessive use of energy drinks
References
9. Centers for Disease Control and Prevention. Data & statistics on Tourette syndrome. Accessed October 2022.

Tourette syndrome and other tic disorders in children and adolescents
In this educational module, Olivia Horner, Dr Tammy Hedderly, and Dr Osman Malik review the aetiology, diagnosis, and management of Tourette syndrome and other tic disorders in children and adolescents.

Tourette syndrome and other tic disorders in children and adolescents
In this educational module, Olivia Horner, Dr Tammy Hedderly, and Dr Osman Malik review the aetiology, diagnosis, and management of Tourette syndrome and other tic disorders in children and adolescents.

OCD in children and adolescents: clinical review


Module description
1.5 CPD hours
In this updated learning module for primary and secondary care healthcare professionals, Jessica Gudgeon and Dr Vibhav Shetty review the diagnosis, pharmacological management, and non-pharmacological management of obsessive compulsive disorder (OCD) in children and adolescents.
Key learning points for healthcare professionals include the epidemiology and aetiology of OCD, how to make a diagnosis of OCD, and the role of cognitive behavioural therapy (CBT) in managing OCD.
For more modules on mental health and psychiatric conditions affecting young people, see the child and adolescent mental health learning plan.
Educational objectives
After taking this activity healthcare professionals should be better able to:
● Identify the contributory factors for OCD
● Screen for OCD
● Advise patients on the pharmacological and non-pharmacological management of OCD
Introduction
Obsessive compulsive disorder (OCD) is a psychiatric disorder characterised by persistent and intrusive thoughts, images and urges (obsessions) and repetitive behaviours (compulsions), as listed below
The ICD-10 diagnostic criteria for OCD in children are similar to those for adults. However, children are less likely to have an insight into their obsessions and compulsions, leading to a possible delay in seeking treatment.
Essential points to remember:
● Causation is poorly understood but it can be biopsychosocial and multifactorial.
● The symptoms typically wax and wane, but often follow a chronic course — causing functional impairment and distress.
● While OCD was previously considered rare in children, the estimated prevalence in children and adolescents is actually 0.25–4%.
● Paediatric OCD is associated with an increased risk of other psychiatric disorders in adulthood.
Scroll within the image below to view more about obsessions vs compulsions1




Obsessions
Definition
Recurrent, intrusive and persistent thoughts, images or urges that cause distress
Common themes
● Contamination
● Fear of harm
● Sexual
● Religious
● Making things ‘just right’
Compulsions
Definition
Repetitive behaviours or mental rituals performed to reduce anxiety
Common themes
● Washing and cleaning
● Checking
● Reassurance seeking
● Repeating
● Ordering and arranging
References
1. Krebs G, Heyman I. Obsessive-compulsive disorder in children and adolescents. Arch Dis Child 2015; 100(5): 495–59.
The precipitators for OCD are variable but can be broadly categorised as follows:
● Genetic: OCD is a highly heritable condition. First-degree relatives and monozygotic twin offspring of patients who have OCD have higher rates of OCD and anxiety disorders.
● Neurobiological: characteristic neuropsychological profiles have been found in children and adults who are diagnosed with OCD.
● Environmental: the role of environmental factors remain unclear, with conflicting evidence regarding environmental triggers such as social isolation and physical abuse.
● Individual: personality traits, such as perfectionism and rigidity, may be predisposing factors. High personal expectations and low self-esteem are also considered risk factors.


PANDAS/PANS subgroup
PANDAS (paediatric autoimmune neuropsychiatric disorders associated with streptococcus) is a term for a subgroup of children who have a sudden onset of OCD symptoms after a streptococcal infection. More recently, the condition has been termed ‘paediatric acute-onset neuropsychiatric syndrome’ (PANS), following suggestions that several pathogenic agents, rather than only streptococcus, might be involved.
The mechanism is unknown and the effectiveness of prophylactic antibiotics remains inconsistent.


Being a perfectionist can predispose a
child/adolescent to develop OCD
(Image credit: Miodrag Ignjatovic/Getty images)

OCD in children and adolescents: clinical review
In this updated learning module, Jessica Gudgeon and Dr Vibhav Shetty review the diagnosis, pharmacological management, and non-pharmacological management of obsessive compulsive disorder (OCD) in children and adolescents.

OCD in children and adolescents: clinical review
In this updated learning module, Jessica Gudgeon and Dr Vibhav Shetty review the diagnosis, pharmacological management, and non-pharmacological management of obsessive compulsive disorder (OCD) in children and adolescents.
Psychotropic medication and renal impairment
1 CPD hour
The prescribing of antipsychotics, antidepressants, and other psychotropic drugs in people with renal impairment is outlined in this CPD module. Pharmacist Michelle Lad looks at the link between renal impairment and mental health conditions, and reviews the potential side-effects of psychotropic drugs in this population.
Educational objectives
After taking this activity healthcare professionals should be better able to:
● The risk of mental health illnesses in people with renal impairment
● The general considerations when using psychotropic drugs in people with renal impairment
● How to safely prescribe and monitor the use of antipsychotics, lithium, and antidepressants

Diagnosis and management of functional seizures
1 CPD hour
In this educational module, Dr Michael Pattrick and Professor Markus Reuber discuss the diagnosis and management of functional seizures (also known as dissociative seizures). They also look at how to distinguish these seizures from other types of transient loss of consciousness, such as epilepsy or syncope.
Educational objectives
After taking this activity healthcare professionals should be better able to:
● The signs and symptoms that can help to determine whether an episode is syncopal, epileptic, or functional/dissociative in nature
● The role of patient history/witness reports in determining the cause of an episode
● Management options for people with functional seizures

Supporting displaced people with mental health conditions
1 CPD hour
In this CPD module for healthcare professionals with an interest in mental health and psychiatry, Professor Cornelius Katona and Dr Cara Katona review how to support refugees, asylum seekers, and undocumented migrants who have mental health conditions.
Educational objectives
After taking this activity healthcare professionals should be better able to:
● The common mental health conditions that affect displaced persons
● The contributory factors for mental health conditions in displaced persons
● The need to understand cultural differences
Autism spectrum disorder: clinical review
1.5 CPD hours
This updated clinical review, by Royal College of General Practitioners autism champion Dr Carole Buckley and Professor Richard Mills, looks at the presentation of autism spectrum disorder and how to support autistic individuals.
Educational objectives
After taking this activity healthcare professionals should be better able to:
● Identify signs that may indicate a diagnosis of ASD
● Be aware of commonly co-occurring conditions such as ADHD, dyspraxia and sleep disorders
● Discuss approaches for supporting autistic individuals with the individual and/or their families
Psychotropic medication and renal impairment
1 CPD hour
The prescribing of antipsychotics, antidepressants, and other psychotropic drugs in people with renal impairment is outlined in this CPD module. Pharmacist Michelle Lad looks at the link between renal impairment and mental health conditions, and reviews the potential side-effects of psychotropic drugs in this population.
Educational objectives
After taking this activity healthcare professionals should be better able to:
● The risk of mental health illnesses in people with renal impairment
● The general considerations when using psychotropic drugs in people with renal impairment
● How to safely prescribe and monitor the use of antipsychotics, lithium, and antidepressants
Diagnosis and management of functional seizures
1 CPD hour
In this educational module, Dr Michael Pattrick and Professor Markus Reuber discuss the diagnosis and management of functional seizures (also known as dissociative seizures). They also look at how to distinguish these seizures from other types of transient loss of consciousness, such as epilepsy or syncope.
Educational objectives
After taking this activity healthcare professionals should be better able to:
● The signs and symptoms that can help to determine whether an episode is syncopal, epileptic, or functional/dissociative in nature
● The role of patient history/witness reports in determining the cause of an episode
● Management options for people with functional seizures
Supporting displaced people with mental health conditions
1 CPD hour
In this CPD module for healthcare professionals with an interest in mental health and psychiatry, Professor Cornelius Katona and Dr Cara Katona review how to support refugees, asylum seekers, and undocumented migrants who have mental health conditions.
Educational objectives
After taking this activity healthcare professionals should be better able to:
● The common mental health conditions that affect displaced persons
● The contributory factors for mental health conditions in displaced persons
● The need to understand cultural differences
Autism spectrum disorder: clinical review
1.5 CPD hours
This updated clinical review, by Royal College of General Practitioners autism champion Dr Carole Buckley and Professor Richard Mills, looks at the presentation of autism spectrum disorder and how to support autistic individuals.
Educational objectives
After taking this activity healthcare professionals should be better able to:
● Identify signs that may indicate a diagnosis of ASD
● Be aware of commonly co-occurring conditions such as ADHD, dyspraxia and sleep disorders
● Discuss approaches for supporting autistic individuals with the individual and/or their families